 |
So-called idiopathic scoliosis |  |
| SKOLIOZA / SCOLIOSIS | (1) So-called idiopathic scoliosis |  POLISH VERSION POLISH VERSION |
Partner / książki / books: 
|
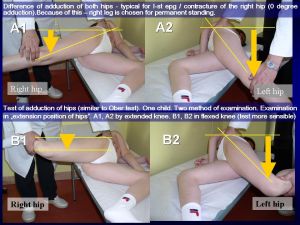
(1) How does the so-called idiopathic scoliosis develop? Biomechanical Etiology. General/Essential/Elementary information about so-called idiopathic scoliosis. In details see lectures in part on left (click point 9) "FOTOS / PHOTOS" / WYKŁADY / LECTURES [1] Biomechanical etiology - connection with hips - explanation of development of spine deformity: A/ In every child with scoliosis - there exists asymmetry of movement of right and left hips. This asymmetry is in connection with "Syndrom of contractures in newborns and babies" - Prof. Hans Mau (Tubingen/Germany) " in German - Siebener [Kontrakturen] Syndrom". What kinds of movements are limited? See below !
B/ In children with scoliosis there exists a limitation of adduction of the right hip or even exists "abduction contracture of the right hip" - important - examination in extension [straight position] of the joint (Karski) - [it is equal with what was described by Prof. Hans Mau as "Haltungsschwache"]. Often (and in every case in I epg - "S" double curve scoliosis and in III epg group - "I" scoliosis - see down) is also limited internal rotation (!), often also limited extension of the right hip.
C/ Because of this asymmetry of movements, there exist biomechanical influences on the pelvis and the spine during gait (!) and also influence going from "the habit to stand permanent 'at ease' on the right leg" in every case of scoliosis.
scoliosis [2] The importance of gait (!) "Gait in scoliosis" & "standing 'at ease' in scoliosis. In Mongolia/Asia no scoliosis, because the children mostly ride on horses - information from Professor Josef HYANEK - (biochemical doctor & pediatrician) in Prague / Czech Republic who was in Mongolia 2 years. Information is given - during Orthopaedic Symposium, October, 2006. Organizer of the Symposium - Professor Ivo Marik.
There is also no scoliosis in blind children. Why? After discussion (letters) with Professor Veikko Avikainen from Finland (Kauppakatu 23 A 17, 40100 Jyvaskyla, Suomi/Finland) and Professor Jacques Boulot (pediatric and adult scoliosis, spinal reconstructive surgery) from 31-400 Toulouse, Rue des Buchers, France - Polyclinique du Parc (discussion on International Orthopaedic Congress in Cairo - 4-9.12.2006) - now I can answer - blind children walk differently than children who see normally and because of this - they do not have scoliosis (see the LECTURE from IRSSD Meeting Liverpool, 2008). Blind children walk without "eye control" but with the big "thinking-muscles control", with careful every step, which changes "the manner of walking". Their walk is with short steps, slowly and with "great caution". So, even in case / in situation of "abduction contracture and external rotation contracture of right hip" it is no scoliosis, because - no "biomechanical influences" occuring during walking/gait. Please, make your own observation on this topic (Karski, December 2006 / January 2007).
[3] Farther explanation of development of scoliosis on the example of "S"- shaped double scoliosis (I-st etiopathological group [epg] of scoliosis. There are important significance of "gait" and "standing position 'at ease' of the right leg" for many years (see up and below - next points):
A/ The limitation / contracture of the right hip leads to movements asymmetry of both hips, next to transmitting asymmetrical loading from the "missing" (restricted) movements of the right hip to the pelvis and to the spine during gait,
B/ This produces rotational deformity of the spine with stiffness and in some children a lordotic deformity (see computer gait analysis in other chapters of this Web Site) of the thoracic spine, making the anterior spinal column longer than the posterior spinal column (first stages in Ist epg - etiopathological group [epg] "S" double curves scoliosis - [3D Deformation] Karski 2001). Some cases in I epg group are "lordoscoliosis". See also the chapter "FOTOS/PHOTOS/WYKŁADY/LECTURES" and next "Badanie/Examination/LECTURES [Pl & Eng]" and here "Computer Gait Analysis" (click on the link on the left).
[4] The importance of "standing 'at ease' in scoliosis. Every child with scoliosis has a permanent habit of standing "at ease" only on the right leg (!) see point [1] / C/.
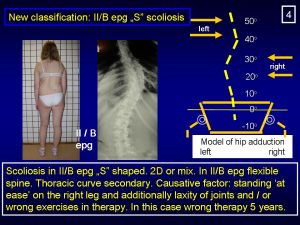
"Standing" is the main cause for "C" scoliosis (II/A etiopatological group - see next chapter) and is also the cause for "S" scoliosis (II/B epg "S" scoliosis) as special sub-type.
In this "S" IInd/B epg - sub-type scoliosis, the thoracic right convex curve is the secondary deformation. This II/B epg "S" sub-types scoliosis - is
The standing "at ease" on the left leg, or on 'the crossed legs', or in the position "uchi hachi ji dachi" or "kiba dachi" (terms from Karate) are safe for the spine and protect before scoliosis.
[5] Scoliosis - is the secondary - not genetic (!) deformity of spine and body (T.Karski - 1995 - 2004/2006/2007/2015).
[6] Short about new clasification of so-called idiopathic scoliosis - general observation and explanation. Observations for approximately 20 years - from a large sample of clinical cases of children (N - 1300 - now 1450 July 2008, now 1950 - July 2015) with scoliosis in all types.
Here (in this chapter) are presented / explaned only connections with "gait" and "standing position 'at ease' on the right leg" and type of scoliosis:
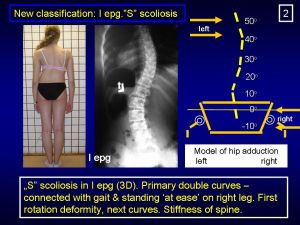
I epg - "S" double curve scoliosis with stiffness of spine and with gibbous costalis, both curves develop at the same time. Influences: "gait" & standing "at ease" only on the right leg. Some cases from I-epg are described as "lordoscoliosis". Progression.
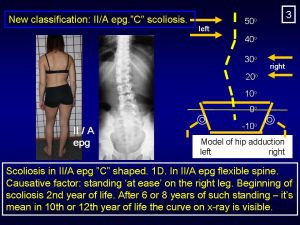
II/A epg - "C" one curve scoliosis. Influences: standing "at ease" only on the right leg since first years of life. No progression or slight.
II/B epg - "S" scoliosis, lumbar curve primary, thoracic curve secondary, without stiffness of spine and without gibbous costalis (or with very small). Influences: standing "at ease" only on the right leg since first years of life, laxity of joints, "wrong"/harmful exercises. Some cases from II/B-epg are described as "kyphoscoliosis". No progression or slight.
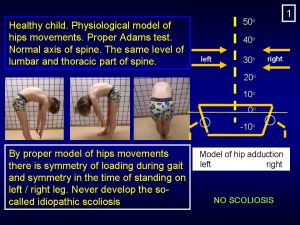
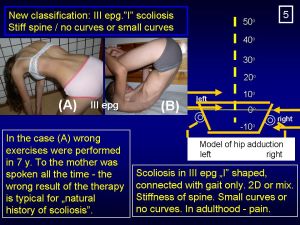
III epg - "I" scoliosis without curves, without gibbous costalis (or small) but with "stiffness of spine". Influences: gait. No progression. There are obviously / of course "mixed cases". More in page [click of left]"(3) "Types of scoliosis" and in many LECTURES. In the pictures down - are presented adduction of hips test, model of hips movements and type of scoliosis.
************* ************* ************* *************
[7] HISTORY / Important dates:
1995 - first lecture about biomechanical etiology of scoliosis on Orthopaedic Congress in Szeged / Hungary),
1997 - confirmation/statement - in clinical material - that all children with scoliosis have the habit to stand "at ease" only on the right leg.
2001 - new classification - description of Ist ["S"], IInd/A ["C"] and IInd/B ["S"] etiopathological group of scoliosis (epg), 2004 - new classification - description of IIIrd etiopathological group of scoliosis (IIIrd epg - "I" scoliosis - deformity of spine without or with a slight curve, without or with a slight gibbous costalis. The main symptom of this type of scoliosis is "stiffness of spine" (rigidity of spine).
2006 (November) : Description of hips model movements and type of scoliosios - ...Confirmation that in IInd etiopathological group of scoliosis (the deformity in this group is connected only with permanent standing position "at ease" only on right leg) can be also the "S" IInd/B epg type of scoliosis In orthopaedic literature there are known "Kyphoscoliosis". Now I can explain - such type of scoliosis belongs to the II/B epg type ("S" scoliosis). The difference between "S" scoliosis in I-epg and "S" scoliosis in II/B-epg is: in I epg - there is stiffness of spine, in II/B epg the spine is flexible. In II/B-epg "S" scoliosis there is no rotation deformity, no stiffness of spine, no rib hump or very small, lumbar curves develop as first, thoracic as second and is always smaller. No progression. In orthopaedic literature this type of scoliosis is also called "kyphoscoliosis". In I-epg "S" double scoliosis - there is first rotation deformity, stiffness of spine, sometimes "lordotic deformity of thoracic part of spine", rib hump - both curves develop at the same time. Typical is progression. In orthopaedic literature some cases in this type of scoliosis is also called "lordoscoliosis".
In October 2006 / January 2007 I described the "biomechanical conditions / model of movements of both hips" in III epg group of scoliosis. Model of movement and type of scoliosis in new classification. 2007 (January): Explanation why the blind children have not scoliosis (!) In January 2007 I was able to answer the question: why the blind children do not have scoliosis? Explanation: the blind children's way of walking is completely different than the children's who see normally. Their walking is without lifting of legs and with a big attention and with every step taken very carefully. Also their way of standing is different - they stand in abduction, with the equal loading of both legs (ophtalmologist remarks - Dr Jola Karska - June 2007). This different way of walking and way of standing protects the blind children from scoliosis (described on 24 February 2008).
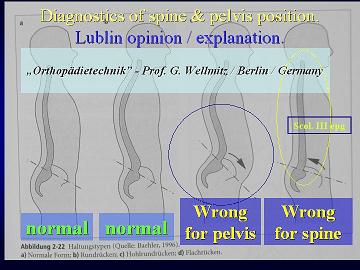
In 2007 (May / June) I found the etiology of "anterior tilt of pelvis" in small children at the age of 2 - 3 - 4 year. The clinical symptoms of "anterior tilt of pelvis" is: hiperlordosis lumbalis, shifting of buttocks to the back, shifting of the stomach to the front. This deformation can be diagnosed by "kneeling test". This wrong position of pelvis causes the wrong (sometimes almost horizontal) position of os sacrum. Such position makes the conjunction of pelvis and sacrum bone less stable - it means - easier development of scoliosis (!) It was also mentioned by Prof. Donat Tylman from Warsaw. What is the cause of "anterior tilt of pelvis" and hyperlordosis in lumbar part of spine? Primary it was thought that it is congenital / genetic deformation / malformation. Such explanation is possible and correct, but in June 2007 I found that this "malposition" of pelvis can be also connected with the "minimal brain damage" [MBD], because in this neuro-muscle disfunction of some children we see shortening of mucles and tendons. By "anterior tilt of pelvis" we see shortening of muscle rectus (one part of m. quadriceps). The shortening of m. rectus can be diagnosed by Elly-Dunkan, or Staheli, or Thom, or "kneeling" test. In history "of mother and child" it is important to ask about pregnacy and delivery period (APGAR). By clinical examination we could see also typical (often only small) extension contracture of spine (functional extensor muscles contracture / shortening), in knees (positive Holt test) and feet (positive QST) [T. Karski]. These children are often - typical example for the ADHD children (Attention Deficit Hyperactivity Disorder). These children (at age of 4 - 10 years) also very like to jump (from the chair, from the table, from trees, from the wall - on the floor / on the ground) - and repeated jumping every day and for many days or weeks is the "cause of Perthes disease". Jumping cause "permanent trauma of femoral head" / "Permenante Traumatisierung des Femurkopfes als Ursache von Perthes Krankheit" (German.) - observed by T. Karski in 1981/1982!!! It is also confirmend in many researches in our Department - 1981 - 2008 (T.Karski,J.Karski, J.Kałakucki, M.Długosz). This knowledge enable us - in Lublin District - effective prophylactics of Perthes Disease (!!!).
In conclusion (the observations from May/June 2007) it is connections (indirect [!]) of CNS in small children and "scoliosis in future". In Minimal Brain Damage (MBD) cases can exist the causes connected with (see picture down): (1) "malposition (wrong position) of pelvis - "anterior tilt of pelvis" [because of shortening of m.quadriceps / m. rectus and other m. flexors of hips]- in consequence makes influences in development of scoliosis (the conjunction of pelvis and sacrum bone is less stable),
(2) "extension contracture of trunk [shortening of soft tissue / m. extensors of trunk] / e.g. extension contracture spine of child" - later 'give rise to' for the danger for I epg scoliosis ("make easy the development of scoliosis in future"),
(3) "general laxity of joints" - and later the danger of progression of every type of scoliosis. According to Prof. Harald Thom from Heidelberg (1972/1973) / later Prof. Thom was in Rummelsberg near to Schwarzenbruck/Nurnberg (1997) - ca. 10% - 20 % of children with cerebral palsy or only with MBD have "the laxity of muscles" (tk - 1972/1973 - 2008). Przykurcz zginaczy bioder i przodopochylenie miednicy ma istotny wpływ na rozwój skoliozy (D. Tylman, T. Karski).
Description of the pictures. Picture 1 and 2 (full pathology)- "kneeling test" - hyperlordosis lumbalis, stomach moved to the front, buttock moved to the back. This position of pelvis makes easy development of scoliosis. The same pathology like children 1 & 2 - "anterior tilt of pelvis" shown on picture No 3 - taken from the book of Prof. G. Wellmitz / Berlin / Germany. In older age "lumbar pain" because of insufficiency of this part of spine - sometimes - "spondylolisis or spondylolisthesis". Picture 3 (small pathology). Picture 4 - normal position of pelvis and spine -axis of trunk, of pelvis and thighs is straight -it means normal / physiological kneeling test" -
Description of the picture 5, 6, 7, 8, 9 - the children in sitting "Polish position" - the spine in straight position. This "extension position of spine" can be connected with bigger or smaller disfunction of CNS in children (MBD - Minimal Brain Damage). Such position of spine can "make more easy the development of scoliosis in future" (obsevations from May / June 2007 - T. Karski).
Laxity of joints and scoliosis. Picture 1 (up left)- Sylwia, born 5.07.1994 - double "S" scoliosis I epg, big progression because of previous "wrong/extension exercises" for one year and because of laxity of joints. Now scoliosis / both curves over 40 degree (Cobb). She is in 2008 in plan for operation (just operated in September 2008). Picture 2 (up right)- Monika, born 1.03.1993 - double "S" scoliosis I epg, in first years moderate progression. Since 7.03.2006 treatment / new exercises in Lublin - additionaly since March 2006 - KARATE. On 14th June 2008 - in clinical and in X-ray examination: decreasing of lumbar curve, stop in progression of thoracic curve. She told me - she is very active in sport in school and additionaly makes karate two years. She is happy because of succes of treatment. Picture 3 (down left) - mother of Monika - no laxity of joints. Picture 4 (down right)- father of Monika - laxity of joints, difference in adduction of hips, scoliosis "C" II/A epg. Never treated. Now "pain in sacro-lumbar part of spine" (on the picture Monika is making the examination of "mother's and father's hand" - author makes all photos). Conclussion - "laxity of joints" in Monika is genetic and coming from father, but mostly "laxity of joints" is neurogenic as described above (!). |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||


















| Data modyfikacji: 2015-08-20 | Strona przygotowana przez Prof. dr med. Tomasza Karskiego | |||
 |
 |